Key Points
- In 2020, nearly 42 million US women had a potential demand for contraceptive services and supplies, and 18.8 million were likely in need of public support for this care.
- Between 2010 and 2020, the number of women with a potential demand for contraceptive care rose steadily. The number of women who were likely in need of public support for this care rose 8% between 2010 and 2016 and then fell 9% between 2016 and 2020, shifts that generally mirror changes in the number of women living in poverty.
- As major components of the Affordable Care Act (ACA) were implemented, the number of women likely in need of public support for contraceptive services who had neither public nor private health insurance fell—from 5.8 million in 2010 to 3.6 million in 2016 and 3.0 million in 2020. States that implemented the ACA’s Medicaid expansion experienced particularly large declines in the numbers of women who were uninsured.
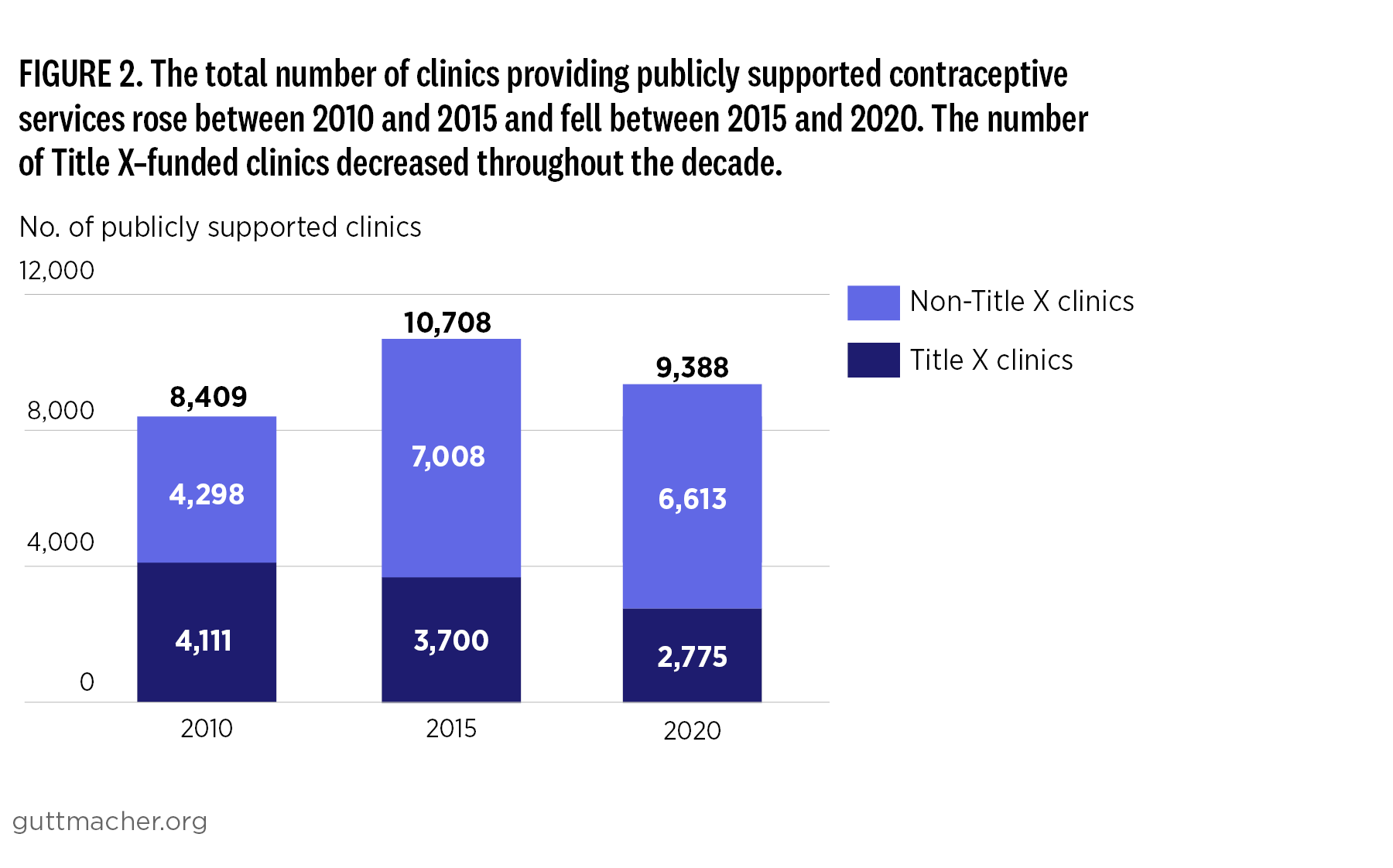
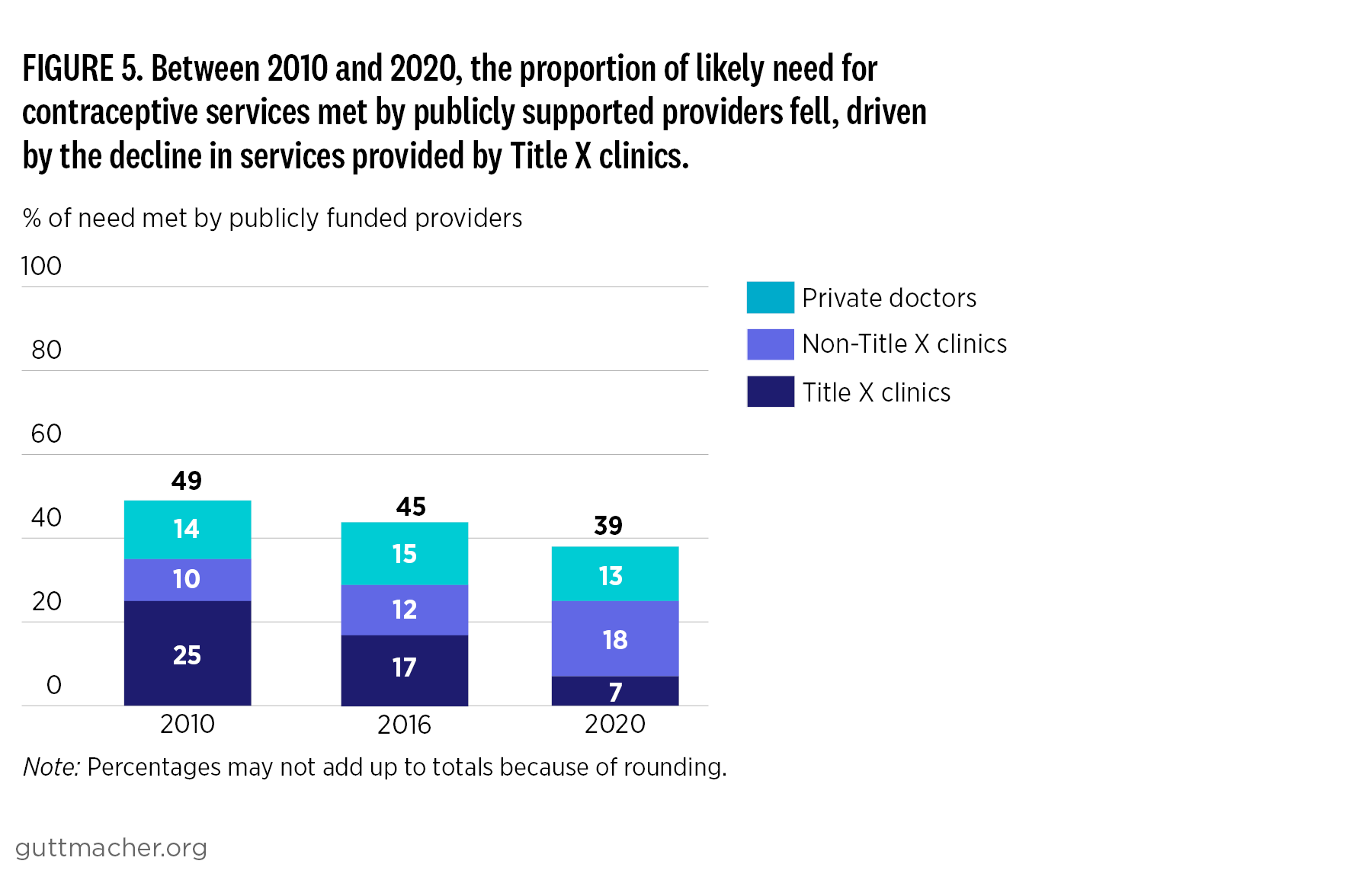
- The overall number of women receiving publicly supported contraceptive services also fell, from 8.9 million in 2010 to 7.2 million in 2020. This drop was due entirely to fewer women obtaining contraceptive care from publicly supported clinics.
- The number of women served by Title X–funded clinics fell over the decade, while the number of women served by clinics not receiving Title X rose dramatically.
- The Trump administration’s “domestic gag rule” and COVID-19 both contributed to large shifts in the publicly funded clinic network between 2015 and 2020. The combined impact of these events appears to have been greater on Title X–funded clinics than on other clinics.